Lately I've been working on how to help therapists strengthen their skills with DBT case formulation and treatment planning. Even though this is for a course on DBT, some of these ideas may be useful to you, regardless of your approach.
Chain Analysis and Mini-Treatment Plans
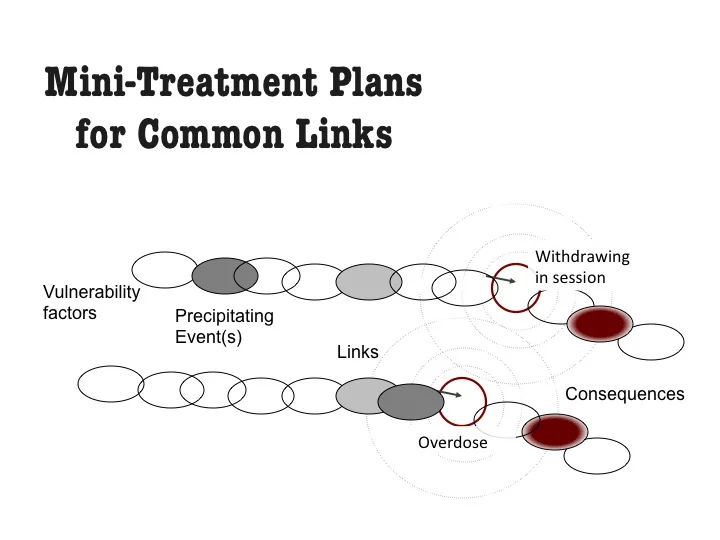
First, to me, case formulation is a shared activity. My client and I develop an understanding of a problem and what to do about it, most often sketching on a white board or piece of paper. In other words, the dreadful part of me at my computer trying to 'write a case formulation' comes WAY later. We start with functional analysis to identify the controlling variables that set off and maintain the problem. All therapies shape awareness of antecedent-behavior-consequences more or less explicitly and in DBT, the particular method is called chain analysis. Taking a specific instance of a problem occurrence, together the client and I figure out:
What exactly is the problem behavior (specific details, intensity, duration)?
When did the problem start? What set off this instance? When did you first know you were heading toward the problem behavior? When was the point of no return?
What made you vulnerable? Why this day/time and not before?
What happened, moment to moment, each thought, feeling, action, event, and body sensation that linked the precipitating event to the problem behavior. Like a movie unfolding, what led to what?
What happened after the problem behavior? Your own and others' immediate reactions?
By repeating this across targeted problems and over time, we can identify those controlling variables that are common, and typical patterns that set off, lead to or maintain the problem behavior.
Then, if we work consistently to change these common links, change happens faster. A positive change made on one link common across problems helps change many related problems. When we identify a common link, then intervention becomes a repeated sequence of Assess-Motivate-Move. We might do self-monitoring of the target or pattern, we'd motivate by linking the target or pattern or intervention to the client's goals and extend this into commitment strategies as needed, then Move! Move can be towards acceptance or toward change, but by default the mini-treatment plan for a target nearly always is some version of behavioral rehearsal-getting the new replacement behavior to happen. I ask myself, 1) what is the alternative preferred behavior to this common problematic link? 2) does the person have the skill? If no, then teach the skill. If yes, then why is the skillful response not showing up? Do emotional responses get in the way? Then do a variant of exposure procedures. Are contingencies problematic? Do contingency management procedures. Problematic cognition or cognitive processes interfering? Try cognitive modification including defusion.
For example, self-invalidation is a common link. Here's a little teaching clip I made to explain self-invalidation and here is a teaching clip on a mini-treatment plan for treating self invalidation.
To me, the big Case Formulation is most useful if it's comprised of these mini-formulations and treatment plans, co-created by therapist and client. (By the way, for those of you doing DBT, here is a DBT case formulation template that might be of help when you have to do a Big Formulation.)
What do you think? How do you approach these sorts of mini-treatment plans and formulations?
* * *
Kelly Koerner, Ph.D., is Creative Director and CEO of the Evidence-Based Practice Institute, where she explores how technology can scale learning and collaboration so practitioners get better clinical outcomes. More information is at www.practiceground.org
She is a clinical psychologist and an expert clinician, clinical supervisor and trainer in Dialectical Behavior Therapy (DBT). She received her Ph.D. from the University of Washington and has specialized training in a number of evidence based treatments. She has served as: Director of Training for Marsha Linehan’s research investigating the efficacy of DBT for suicidal and drug abusing individuals with borderline personality disorder; Creative Director at Behavioral Tech Research where she developed e-learning and other technology based methods to disseminate evidence-based practices; and co-founder and first CEO of Behavioral Tech, a company that provides training in DBT.
Her most recent publications include Doing Dialectical Behavior Therapy: A Practical Guide (Guides to Individualized Evidence-Based Treatment) and Dialectical Behavior Therapy in Clinical Practice: Applications across Disorders and Settings.
Source: Kelly Koerner